



In an interview on CNN’s “State of the Union,” Virginia Lt. Gov.-Elect Winsome Sears spread misinformation about COVID-19 vaccines that we have previously debunked.
CNN Host Dana Bash, Nov. 21: So, why is it OK to mandate childhood vaccines in Virginia for so many diseases, but not COVID?
Sears: Well, let’s ask ourselves. And I’m not saying yea or nay. Let’s ask ourselves, if the purpose of the COVID vaccine is to prevent us from getting COVID, then why is it that those who have had COVID must get the vaccine? The one doesn’t follow the other.
Sears, a Republican who won the Nov. 3 election and will become the state’s first female lieutenant governor, argues that vaccine mandates shouldn’t apply to those who have already been infected COVID-19. But, as the Centers for Disease Control and Prevention has said, people who’ve already had COVID-19 should be vaccinated for two reasons:
- “Research has not yet shown how long you are protected from getting COVID-19 again after you recover from COVID-19.
- “Vaccination helps protect you even if you’ve already had COVID-19.”
 As we have explained on other occasions, a growing body of research shows that COVID-19 vaccines provide additional protection for those who have been previously infected with SARS-CoV-2, the virus that causes COVID-19. The Centers for Disease Control and Prevention, in fact, recommends that people get vaccinated even if they had COVID-19.
As we have explained on other occasions, a growing body of research shows that COVID-19 vaccines provide additional protection for those who have been previously infected with SARS-CoV-2, the virus that causes COVID-19. The Centers for Disease Control and Prevention, in fact, recommends that people get vaccinated even if they had COVID-19.
For more, see “Vaccines Benefit Those Who Have Had COVID-19, Contrary to Viral Posts.”
Vaccines Not 100% Effective
Sears: But let me ask you this question. If you have the mask on, then why does somebody else have to wear the mask? You have got the mask. You have got the vaccine. My God, you’re fully protected. You’re armored.
No vaccine is 100% effective, and masks aren’t foolproof, so it’s wrong to claim that someone who is vaccinated and wearing a mask is “fully protected” or “armored” against COVID-19.
It’s true that those who are unvaccinated were nearly six times more likely to become infected with COVID-19 in September than those who have been fully vaccinated, according to the CDC’s data on rates of COVID-19 by vaccination status. But, as the CDC chart below shows, that doesn’t mean there aren’t breakthrough infections, which occur in fully vaccinated people.
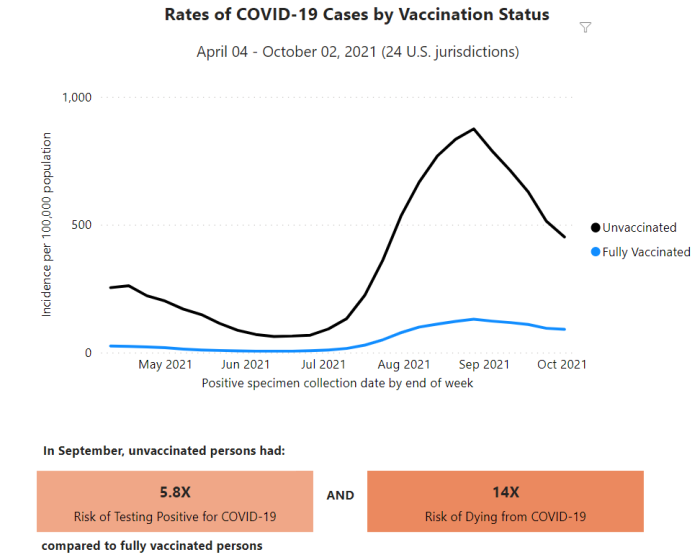
More recent data show that, as of the week ending Oct. 2, there were 91 COVID-19 cases per 100,000 population among the vaccinated and about 452 cases per 100,000 among the unvaccinated.
And while studies support the premise that properly fitted masks can limit the transmission of SARS-CoV-2, they do not eliminate the transmission entirely. The CDC recommends using face masks along with other mitigation measures, such as social distancing, to protect against illness.
For more, see our SciCheck stories “The Evolving Science of Face Masks and COVID-19,” “A Guide to Moderna’s COVID-19 Vaccine,“ “A Guide to Pfizer/BioNTech’s COVID-19 Vaccine” and “A Guide to Johnson & Johnson’s COVID-19 Vaccine.”
Distorting Remarks of Biden, Harris on Vaccines
Sears: In fact, our president, President Biden, and Vice President Harris themselves both said they would not trust any vaccine that was developed by the Trump administration. That was before their election. After their election, they were singing a different song.
We debunked this once before when then-President Donald Trump during the 2020 presidential election charged Biden and his running mate, Harris, with spreading “anti-vaccine conspiracy theories.” At the time, there was concern among some in the medical and research communities that Trump would demand the release of a vaccine against COVID-19 prior to the Nov. 3 election, and before it had been proven safe and effective.
Both Harris and Biden said they would trust a vaccine authorized prior to the election, if scientists independently determined it was safe and effective.
In a CNN interview that aired Sept. 6, 2020, Harris said: “I will say that I would not trust Donald Trump. And it would have to be a credible source of information that talks about the efficacy and the reliability of whatever he’s talking about. I will not take his word for it.”
Later in the interview, Harris said that she would trust National Institute of Allergy and Infectious Diseases Director Dr. Anthony Fauci.
Similarly, Biden was asked on Sept. 7, 2020, whether he’d take a COVID-19 vaccine before the election. “I would want to see what the scientists said,” he replied. “I want full transparency on a vaccine. One of the problems is the way [Trump] is playing with politics. He’s said so many things that aren’t true, I’m worried if we do have a really good vaccine, people are going to be reluctant to take it. And so he’s undermining public confidence.”
Both politicians were vaccinated after the election, but while Trump was still in office. Biden received his first dose of the Pfizer/BioNTech vaccine on Dec. 21, 2020, and Harris got her first shot several days later on Dec. 29.
For more, see “Trump Exaggerates Progress, Credit on Future COVID-19 Vaccine.”
Serious Adverse Events Are Rare
Sears: We know — and, by the way, media, they’re not telling us that people are suffering as a result of getting the vaccine, that they have all kinds of problems. I understand it might be the minuscule. But when you’re the one out of 30,000 that gets it, it’s important to you. So we need to tell the good, the bad and the ugly about the vaccine.
Overall, more than 450 million vaccine doses have been administered in the U.S., so far. But, in this remark, Sears exaggerates the rate of serious adverse events from vaccines. And, as we’ve explained before, the most common side effects of the COVID-19 vaccines includeinjection site pain, fatigue, headache, muscle pain and fever.
Sears is referring to very rare cases when the vaccines may cause more serious problems — such as anaphylaxis, an allergic reaction that “can occur after any kind of vaccination,” according to the CDC. In the case of the COVID-19 vaccines, anaphylaxis has occurred in 2 to 5 people per million, the CDC said, and “healthcare providers can effectively and immediately treat the reaction.”
The Johnson & Johnson vaccine is associated with an increased risk of the neurological disorder Guillain-Barré Syndrome and a blood-clotting disorder known as thrombosis with thrombocytopenia syndrome, or TTS, which occurs mostly in women under 50 years old, according to the Food and Drug Administration.
“As of November 17, 2021, more than 16.2 million doses of the J&J/Janssen COVID-19 Vaccine have been given in the United States,” the CDC said. “CDC and FDA identified 54 confirmed reports of people who got the J&J/Janssen COVID-19 Vaccine and later developed TTS. VAERS [Vaccine Adverse Event Reporting System] reports have identified six deaths that have been caused by or directly attributed to TTS following J&J/Janssen COVID-19 Vaccination.”
There is also emerging evidence that the Pfizer/BioNTech and Moderna mRNA vaccines may very rarely cause inflammation of the heart muscle (myocarditis) or of the surrounding lining (pericarditis), particularly in young men. As of Nov. 17, the CDC and FDA have confirmed 1,822 reports of myocarditis or pericarditis.
These rare serious adverse events have been widely covered in the media, contrary to Sears’ claim. In one case, the FDA and CDC recommended a brief “pause in the use” of the Johnson & Johnson vaccine while it investigated reports of the blood-clotting syndrome — an unusual step that was heavily covered by news outlets.
Sears acknowledged that serious adverse events are “minuscule,” but then she adds that “one out of 30,000” people experience such serious problems. There is no evidence that any rate of adverse events is that high in the general population, as numbers above show. But it may be true for subpopulations – such as the reported incidence for myocarditis for younger men.
In a vaccine safety update presented by the CDC’s Vaccine Safety Team to the Advisory Committee on Immunization Practices on Oct. 21, Dr. Tom Shimabukuro provided data on myocarditis and myocarditis with pericarditis and wrote that the risk of myocarditis is “strongly dependent on patient age and sex.”
For example, Shimabukuro, head of the CDC’s Vaccine Safety Team, wrote this about the data from the military health system: “Overall rate of myocarditis within 7 days of vaccination is 10 cases per million doses, but risk is strongly dependent on patient age and sex, and vaccine dose and type; rate of myocarditis in younger (under age 20) males after 2nd dose mRNA vaccine is [greater than] 100 cases per million doses.”
For this reason, the fact sheets for both mRNA vaccines have been revised to contain a warning that reads: “Myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the lining outside the heart) have occurred in some people who have received the vaccine, more commonly in males under 40 years of age than among females and older males. In most of these people, symptoms began within a few days following receipt of the second dose of vaccine. The chance of having this occur is very low. You should seek medical attention right away if you have any of the following symptoms after receiving the vaccine: chest pain, shortness of breath, feelings of a fast-beating, fluttering or pounding heart.”
It is important to note, however, that COVID-19 and other viruses can also cause myocarditis. A study published by the CDC in early September said “patients with COVID-19 had nearly 16 times the risk for myocarditis compared with patients who did not have COVID-19, and risk varied by sex and age.” The authors also said that the study supports CDC’s earlier determination that the benefits of COVID-19 vaccination outweigh the risks “in all populations, including adolescents and young adults.”
For more, see “How safe are the vaccines?“
Editor’s note: SciCheck’s COVID-19/Vaccination Project is made possible by a grant from the Robert Wood Johnson Foundation. The foundation has no control over our editorial decisions, and the views expressed in our articles do not necessarily reflect the views of the foundation. The goal of the project is to increase exposure to accurate information about COVID-19 and vaccines, while decreasing the impact of misinformation.











{kind=link}